 CHOLESTEROL PILLS, statins, -Pravachol, Lipitor, Zocor, Mevacor, Lescol, Crestor- '..if diet and exercise alone are not enough..' make part of a lab report look 'better'. This makes families poorer and less concerned about food choices while most doctors are not yet blamed for prescribing them. They hardly raise HDL and slash the production of CoQ10 by the same % as LDL, forcing heart, in fact all cells, to work with less energy and more 'free radical' damage. Their limited effect is clearly not from cholesterol lowering but most probably from imitating (cheap and usually safe) nitroglycerin (click on picture to the left) and possibly by reducing inflammation, as would (cheap but not always safe) aspirin, omega-3 fish oil in pills, and many vitamins in a multivitamin, including E).
Those doctors aware of the fact that the statin studies can be explained by their nitroglycerin mimicking effect (and thus less non-fatal angina [heart pain] and angina driven non-fatal benefit) find the concept that they may have been wrong about cholesterol too terrible to contemplate, yet that is what most studies show, including all Lipitor and Crestor (atorva- and rosuva-statin) studies.
Stanol / sterol margarines, policosanol, gugulipid, dextrothyroxine, estrogen, ezetimibe [Zetia, Ezetrol, part of Vytorin (Inegy) -click for warning] and 'killer' fibrates and torcetrapib all 'manage cholesterol' in various ways but have never shown to save lives,
a fact certain for Lipitor.
Some statin fine-print warns "The effects of ... on cardio vascular morbidity [illness] or mortality [death] ... have not [!] been established." And: "Significant decreases in circulating ubiquinone [CoQ10] levels in patients treated with X or other statins have been observed [happens in all users, and this does]
.. lead to impaired cardiac function [= heart failure, nerve death]
..".
As shown on this page, worrying about cholesterol is by far THE least health and cost effective way of dealing with existing artery decline. THE fastest and effective way is getting about 1 g/day of fish oil and 2 g/d of plant based omega-3 and, probably, taking the recommended amount of magnesium, not less than 400 mg/day. Back to the distraction of cholesterol and its drugs:
 Statin simple summary:
1. Good: statins imitate nitroglycerin, resulting in less non-fatal chest pain ('stable' angina) and thus hospital visit and thus about 20-45% fewer stents. Example: Lipitor in the ASCOT study, and now the 2008 JUPITER study also with fewer stents but also zero cardiac deaths prevented after 17,000 years of Crestor use!! Even the FDA: "There was no statistically significant reduction seen for cardiovascular death .."
BETTER: To avoid 90% stents and bypasses, not just 20 or 45%, when having a heart attack, first go to a close and small hospital that cannot "go in" and statistically survival at 6 months is 14% better. 'Planned' balloon angioplasty or stents also do not prevent heart attacks, make you live longer or life quality better (COURAGE study);
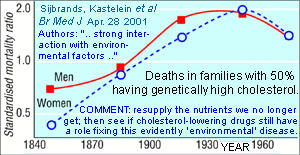
2. No effect: from changes to cholesterol [lipids] however 'familial' (genetically high) patients may be different but the science is not complete;
3. Always bad: pain (joints, weakness, muscle damage), 'senior moments' and memory [try switching to niacin instead!], less CoQ10 (energy), more Lp(a), birth defects, bleeding strokes, poor nerve function (myelin sheath repair / multiple sclerosis), probably cancer and, as per the FDA, diabetes.
4. Scary ads & faulty science [Zocor, Vytorin and the Pfizer feet in the morgue fear of death campaign called 'unethical' by the World Health Organization]
5. Don't prolong survival in most high-risk groups and diabetics and never in women. |
  Massive benefits proclaims Oxford University about its Heart Protection Study. 75% of heart attacks still happen and 110,000 Zocor (simvastatin) pills to postpone one death and this only in men. The next study claiming benefit in high-risk elderly, Pravachol's PROSPER had 28 fewer heart but 24 more cancer deaths and more 'new' cancers in each of 4 years in a group with 52 fewer smokers. Next, zero 'anything' was found in Pravachol's ALLHAT in high-risk North Americans: 1 death postponed per 1.1 million $3 pills taken! Next was Lipitor's ASCOT also without mortality benefit (2nd graph from top). From 10 years ago: cholesterol lowering by any means caused 150 more deaths per 100,000 patient-years of intervention. Cheers. No statin benefit in 'primary' prevention in 2003: click on the right picture.
Massive benefits proclaims Oxford University about its Heart Protection Study. 75% of heart attacks still happen and 110,000 Zocor (simvastatin) pills to postpone one death and this only in men. The next study claiming benefit in high-risk elderly, Pravachol's PROSPER had 28 fewer heart but 24 more cancer deaths and more 'new' cancers in each of 4 years in a group with 52 fewer smokers. Next, zero 'anything' was found in Pravachol's ALLHAT in high-risk North Americans: 1 death postponed per 1.1 million $3 pills taken! Next was Lipitor's ASCOT also without mortality benefit (2nd graph from top). From 10 years ago: cholesterol lowering by any means caused 150 more deaths per 100,000 patient-years of intervention. Cheers. No statin benefit in 'primary' prevention in 2003: click on the right picture.
|
 "Ask your doctor if "Rx" is right for you" prompt the ads but vital information is hidden from you and your doctor. This paves the way for after-the-damage criminal investigations and
lawsuits. Statins, fibrates and high intakes of the common cholesterol-lowering polyunsaturated omega-6 'vegetable' oils (like corn) are linked to more cancer, as is just plain low cholesterol. "Ask your doctor if "Rx" is right for you" prompt the ads but vital information is hidden from you and your doctor. This paves the way for after-the-damage criminal investigations and
lawsuits. Statins, fibrates and high intakes of the common cholesterol-lowering polyunsaturated omega-6 'vegetable' oils (like corn) are linked to more cancer, as is just plain low cholesterol.  Canadian ads but not U.S. ads warn that statins lower CoQ10; there's your muscle and nerve pain, and lack of energy. Fewer studies were done on women and elderly, groups where high LDL has no evident link to mortality [low HDL does have such link, but HDL is best raised by, for example, exercise, moderate alcohol use or mega-niacin with -or it will raise homocysteine- a multivitamin]. No mortality studies were done in people taking a good multi, whole foods and omega-3 oil.
Many B-vitamin (homocysteine) trials are now being done but some are in people where prevention is rather (too) late, some were destined for failure (VISP) and many are set-up to have statins share the credit. The latter paves the way for combination therapy: statins + niacin and/or aspirin and/or fish oil and/or multi-B-vitamins ... if statins alone are not enough ... Canadian ads but not U.S. ads warn that statins lower CoQ10; there's your muscle and nerve pain, and lack of energy. Fewer studies were done on women and elderly, groups where high LDL has no evident link to mortality [low HDL does have such link, but HDL is best raised by, for example, exercise, moderate alcohol use or mega-niacin with -or it will raise homocysteine- a multivitamin]. No mortality studies were done in people taking a good multi, whole foods and omega-3 oil.
Many B-vitamin (homocysteine) trials are now being done but some are in people where prevention is rather (too) late, some were destined for failure (VISP) and many are set-up to have statins share the credit. The latter paves the way for combination therapy: statins + niacin and/or aspirin and/or fish oil and/or multi-B-vitamins ... if statins alone are not enough ...
 A TV ad exclaims: 'Lipitor did it, the lower numbers you're looking for.' Then, a small banner: "Lipitor has not been shown to prevent heart disease ... " Isn't that what people expect when taking the drug? In 2005, Lipitor ads no longer mentioned heart disease, it simply 'treats' (bad) cholesterol, a concept created by the drug and food industry. In 2011 they again mention (non fatal) heart issues but avoid the fact nobody lived longer: the "Don't Kid Yourself" campaign. A TV couple: 'Oh, Jessie, I love you too!' [...Zocor, Be There!]. Up to 87% of Baycol* users drop to 'target levels' but 'effects on disease and death have not been established.' Why not real wellness goals such as less illness, fewer doctors visits or more time with friends?
A TV ad exclaims: 'Lipitor did it, the lower numbers you're looking for.' Then, a small banner: "Lipitor has not been shown to prevent heart disease ... " Isn't that what people expect when taking the drug? In 2005, Lipitor ads no longer mentioned heart disease, it simply 'treats' (bad) cholesterol, a concept created by the drug and food industry. In 2011 they again mention (non fatal) heart issues but avoid the fact nobody lived longer: the "Don't Kid Yourself" campaign. A TV couple: 'Oh, Jessie, I love you too!' [...Zocor, Be There!]. Up to 87% of Baycol* users drop to 'target levels' but 'effects on disease and death have not been established.' Why not real wellness goals such as less illness, fewer doctors visits or more time with friends?
Eight authors of the U.S. ATP III 2004 treatment guideline update got money from average 10 drug companies; one, a NIH gov't employee, got $114,000 + 'stock options' from industry. The 9th author is employed with the job to '..increase the proportion [.. of Americans] who adhere to their cholesterol-lowering regimen.' And, oeps, they forgot the largest statin study ever, J-LIT (graphs at end). More on conflicts of interest. Could the brilliant beauty of a drug (industry) blind a well meaning doctor or is it fear of not following 'guidelines'? *)Baycol (Lipobay) was withdrawn for causing unexpected deaths: here's an important comment about all statins.
A site for side effects: StoppedOurStatins. A scary YouTube: YouTube.
   How about Pravachol? Two analysis by the Journal Club here and here; some high risk participant would have to be treated for over 200 years at a drug cost of $200 000 to prevent one cardiac 'event'. The WOSCOPS study selected 6600 men out of 160 000 and treated half. After 5 years and 30% giving up on the drug total deaths were not quite statistically different. The CARE study found, in patients with prior heart attacks '.. no significant differences in overall mortality ..' [1.6 per 1000 years of drug use, a statistical fluke.] NEJM; 99-4-8:1115 about a 3rd study (LIPID): '[Pravachol] has no particular advantage over placebo [dummy-pill].' Finally, the truly massive ALLHAT study found 'zip' in any health department!
How about Pravachol? Two analysis by the Journal Club here and here; some high risk participant would have to be treated for over 200 years at a drug cost of $200 000 to prevent one cardiac 'event'. The WOSCOPS study selected 6600 men out of 160 000 and treated half. After 5 years and 30% giving up on the drug total deaths were not quite statistically different. The CARE study found, in patients with prior heart attacks '.. no significant differences in overall mortality ..' [1.6 per 1000 years of drug use, a statistical fluke.] NEJM; 99-4-8:1115 about a 3rd study (LIPID): '[Pravachol] has no particular advantage over placebo [dummy-pill].' Finally, the truly massive ALLHAT study found 'zip' in any health department!
 The Mevacor (lovastatin) EXCEL trial had, with 89% probability, 2.75x more deaths (97% cardio-vascular) after 2 million pills were swallowed (11% fewer heart attacks, 40% more cancer); then, dumping 97% of the placebo group, Merck continued but without the risk of the drug proving conclusively to be more fatal than a dummy pill (dead patients kill drugs). Then, after 3 times more Mevacor pills, the AFCAPS / TexCAPS trial ended with 3 more drug deaths. Next, Merck's 1st Zocor study (4S) killed 3 more women but saved men, but with unexplained anomalies in the mortality curves starting at 18 months. The Mevacor (lovastatin) EXCEL trial had, with 89% probability, 2.75x more deaths (97% cardio-vascular) after 2 million pills were swallowed (11% fewer heart attacks, 40% more cancer); then, dumping 97% of the placebo group, Merck continued but without the risk of the drug proving conclusively to be more fatal than a dummy pill (dead patients kill drugs). Then, after 3 times more Mevacor pills, the AFCAPS / TexCAPS trial ended with 3 more drug deaths. Next, Merck's 1st Zocor study (4S) killed 3 more women but saved men, but with unexplained anomalies in the mortality curves starting at 18 months.
  Problem at OXFORD: Sir Peto (left) and Dr. Collins refuse to publish the Heart Protection Study mortality curves in men, women, diabetic or not. In 1992 both wanted 'total mortality' trials. They did such study but hide the generated mortality data. In 2004 Dr. Collins suggested they would release these data but did not. In April 2007, author Dr. Baigent said it would be 'inappropriate' to publish these data and author Dr. Sleight: 'It is not my decision, but it looks like that.' [not releasing the data about deaths that he himself favoured releasing]. Their client Merck is also mum about deaths but as always, women did not benefit. If you're a diabetic women with a 75% chance to die from blood vessel diseases, would you not like to know how many days of life you might statistically gain or lose taking Zocor (simvastatin) for 5 years? That is not an 'inappropriate' question but a real one and even more so when balancing money for food or drugs. Male (only?) benefit appears at 1.3 and ends near 4 years of use, something spookily similar to what was found in the 4S study with the same drug.
Next, Merck contractor Oxford got another 78m$ for a new 5 year study with simvastatin, Zocor, plus 2 other drugs including one, laropiprant, with a non cardiac (marketing) benefit lasting less than 8 weeks but with unknown long-term prostaglandin [D2] consequences. The 3rd drug is not just 2 grams of plain niacin (mega-vitamin B-3) but a 20x more expensive pharma version of the mail-ordered bulk generic vitamin. The combo has the trade name Cordaptive® and it comes without the other B vitamins that prevent niacin from raising toxic homocysteine.
Some Oxford employees consult and speak for drug companies for free and accept travel perks. Fine, but then at least release all study data and most certainly those about deaths. Pharma pays Oxford 4 weeks of projected sales (they call it a 'grant'); Oxford's name: priceless [for now]. Ironically, they called that study 'thrive'. Same size as HPS but starting anew avoids the increasing mortality rate found after 5 years in 4S.
2013: Study halted, and the drug combo withdrawn. Was it the funny "D2" drug? We'll never know.

20% of first-time Zocor users were motivated by cholesterol fear instilled by a football coach (Merck annual report). Pfizer also uses sports figures and, before Feb. 25 2008,
a doctor who had never practiced.
A shocking statement on the 2007 ALLHAT study website: "..trials demonstrating a reduction in coronary heart disease from cholesterol lowering
 have not [sic] demonstrated a net reduction in mortality." MedlinePlus about ALLHAT: "..people taking pravastatin were no less likely to die or develop heart disease than people receiving usual care." have not [sic] demonstrated a net reduction in mortality." MedlinePlus about ALLHAT: "..people taking pravastatin were no less likely to die or develop heart disease than people receiving usual care."
 The Lipitor (Tahor in France, atorvastatin in any language) mortality curves still touch at mean study end in the ASCOT study after 10 million drug or dummy pills; 5 more 'vascular' deaths in those with diabetes and 2 more heart attacks in women on Lipitor. Next, there were 5 more deaths on Lipitor than on dummy pills in the 5 year SPARCL study (stroke patients) and 2 more in the 4 year ASPEN study (in diabetics). Pfizer initially refused to reveal data about deaths for 49 in-house studies. Reversing itself in a letter, the data suggest higher than expected deaths compared with placebo. Not ever saving lives in a fatal disease with the world's top selling drug is a sad little known reality. Some professors propose the term pharmageddon. The Lipitor (Tahor in France, atorvastatin in any language) mortality curves still touch at mean study end in the ASCOT study after 10 million drug or dummy pills; 5 more 'vascular' deaths in those with diabetes and 2 more heart attacks in women on Lipitor. Next, there were 5 more deaths on Lipitor than on dummy pills in the 5 year SPARCL study (stroke patients) and 2 more in the 4 year ASPEN study (in diabetics). Pfizer initially refused to reveal data about deaths for 49 in-house studies. Reversing itself in a letter, the data suggest higher than expected deaths compared with placebo. Not ever saving lives in a fatal disease with the world's top selling drug is a sad little known reality. Some professors propose the term pharmageddon.
 Statins aren't cholesterol but mevalonate lowering 'therapy'. This mother-molecule also makes CoQ10 and other vital stuff with names like isoprene [it takes 10 to make Q10, 6 to make cholesterol], farnesyl, geranyl, dolichol and squalene. Similarly, aspirin is not simply 'anti-clot therapy', it rearranges all fat-based 'house keeping', pain and signal machinery. Statins and aspirin hamper (inhibit) fundamental body processes. Whatever good necessarily comes with the bad. On the other hand, niacin promotes over 300 reactions and has few harmful effects since it stimulates body processes, like all vitamins. Niacin must be taken with a multi-B-vitamin or it will raise homocysteine. It is just a partial answer to heart disease and has other benefits but niacin did prevent heart attacks and did save lives; 2006 update. Statins aren't cholesterol but mevalonate lowering 'therapy'. This mother-molecule also makes CoQ10 and other vital stuff with names like isoprene [it takes 10 to make Q10, 6 to make cholesterol], farnesyl, geranyl, dolichol and squalene. Similarly, aspirin is not simply 'anti-clot therapy', it rearranges all fat-based 'house keeping', pain and signal machinery. Statins and aspirin hamper (inhibit) fundamental body processes. Whatever good necessarily comes with the bad. On the other hand, niacin promotes over 300 reactions and has few harmful effects since it stimulates body processes, like all vitamins. Niacin must be taken with a multi-B-vitamin or it will raise homocysteine. It is just a partial answer to heart disease and has other benefits but niacin did prevent heart attacks and did save lives; 2006 update.
|
Bottom Line: At 10 - 36x the price of generic niacin (1000 grams for $45 or 80¢ per week at PureBulk)*, in some types of (mainly male and non-congestive) heart patients, some statins may reduce the risk of "events" by one fifth [probably not "deaths", and you have to scrape the statistical barrel]. This leaves
no less than 4/5ths of the risk. To deal with the larger under lying problem, remember that fat substitutions have proven of no value, apart from those involving omega-3 oils, and that whole-foods and supplements cheaply lower most risk factors -and survival chances. *(tel. 1.800.544.4440 or 1.954.766.8433; product 94.) |
A doctor prescribing statin and not first niacin plus a good multi vitamin, without tracking homocysteine and Lp(a), and without replacement CoQ10, canola and fish omega-3 (pills) and likely a magnesium supplement is practicing incomplete medicine. |
|
 C27·H45·OH -
HIGH CHOLESTEROL, a likely survival benefit prior to refined foods and you'd have to eat almost 20 eggs to absorb what you make each day. The famed Framingham study found better thinking at high cholesterol while
decreasing levels after age 50 predicted more heart disease deaths!
C27·H45·OH -
HIGH CHOLESTEROL, a likely survival benefit prior to refined foods and you'd have to eat almost 20 eggs to absorb what you make each day. The famed Framingham study found better thinking at high cholesterol while
decreasing levels after age 50 predicted more heart disease deaths!
 Studies show that lowering cholesterol with
Studies show that lowering cholesterol with